History and Biology of Neisseria meningitidis
History of Neisseria meningitidis
Neisseria meningitidis, also known as meningococcus, is a Gram-negative diplococcus bacterium, with a “coffee-bean” shape. It was first identified in 1887 by Weichselbaum, although outbreaks of possible meningococcal meningitis had been reported since 1805 in Europe. By the beginning of the 20th century outbreaks were also reported in Africa.

Outbreaks are often seen in military camps, university campus as well as in the African region known as the “Meningitis Belt”.
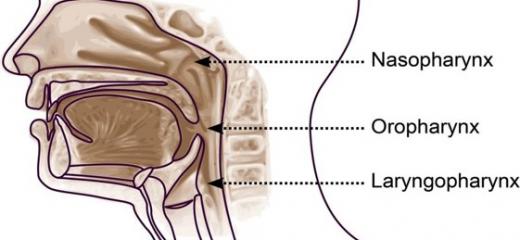
Humans are the only natural host. The bacterium can live transiently in the upper respiratory tract (nasopharynx and oropharynx) of healthy individuals without causing disease (asymptomatic carriage). In susceptible individuals the meningococcus can cause meningitis and meningococcemia, a life threatening type of sepsis (or blood poisoning) that in its more dramatic presentation can lead to limb amputation and death.

Edited from pixabay.com
Biology
Neisseria meningitidis can be capsulated or not, but strains causing disease are often encapsulated.
Virulence factors that enable the meningococcus to evade the immune system include the endotoxin, pili and the capsule polysaccharide. The capsule antigens are also used as targets for vaccines.
Based on capsular polysaccharides, Neisseria meningitidis can be classified into 12 serogroups, 6 of which are responsible for global epidemics, namely: A, B, C, W, X, Y. The meningococcus can also be classified by serotype, serosubtype, and immunotype.
History of meningococcal meningitis in the African Meningitis Belt
Neisseria meningitis is the main pathogen responsible for meningitis epidemics during the dry season in the Sub-Saharan African region, known as the “African Meningitis Belt”.
It is believed that the meningococcus was introduced in West Africa by pilgrims in the end of the 19th century.
First reports of epidemics are from 1905, with an outbreak of meningitis in northern Nigeria, where diplococcus were isolated from a cerebrospinal fluid sample.
In 1906 an outbreak of meningitis was observed in Ghana, at the time with no available effective treatment, fatality rate was as high as 80%. Even now, up to 20% of survivors are left deaf, with epilepsy and other neurological disorders.
Following the 1905 and 1906 outbreaks, many others were identified in the African Belt region, in Niger, Burkina Faso, Mali, Guinea, mainly due to serogroup A.
In 1996, the largest outbreak ever reported in the region was registered. It culminated in 1997, with at least 250 000 cases and 25 000 deaths.
At the time, reactive vaccination with polysaccharide vaccines had already been in place since the 1970s. This epidemic prompted the development of an affordable serogroup A conjugated vaccine for the African meningitis belt, which was introduced in the region in 2010.
To learn more about Neisseria meningitidis and meningococcal vaccines click on the links below.
Other resources can be found here Back to top